Phone
+61 8 8267 2200
Fax
+61 8 8267 5664
Personal Email
In Emergency
0418 829 207
Most stones in the lower and mid ureter can be accessed with the rigid ureteroscope and most stones in the upper ureter and kidney can be accessed with the flexible ureteroscope, long thin telescopes passed up the urethra through the bladder and into the ureter. Multiple or larger stones in the kidney and sometimes upper ureter are more efficiently dealt with by percutaneous surgery.
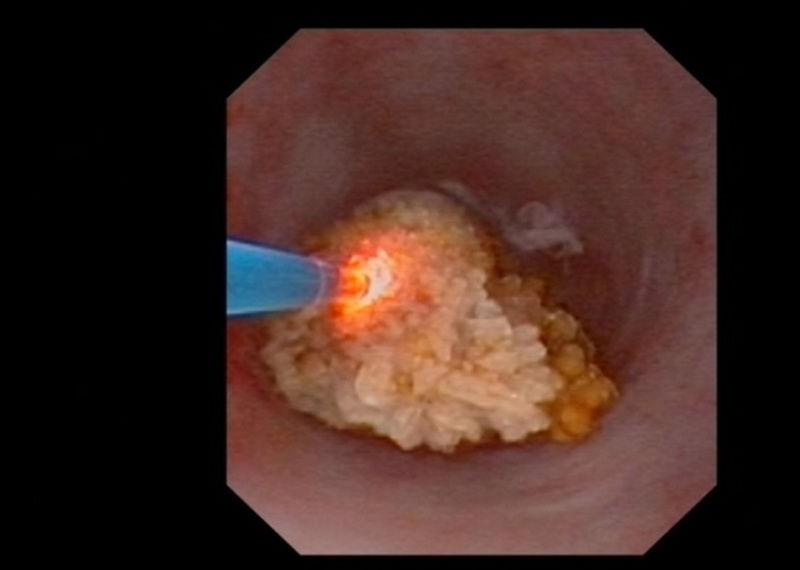
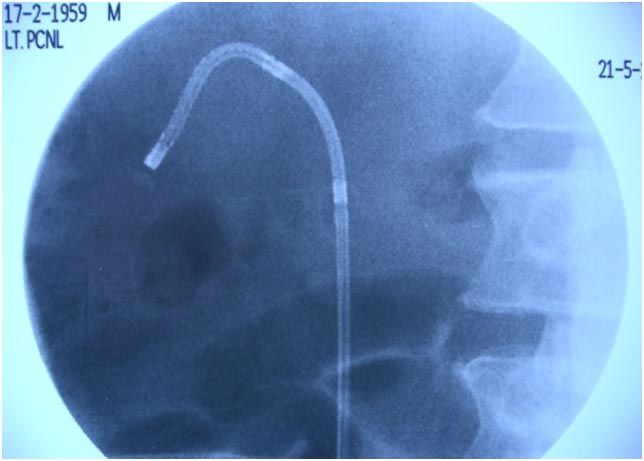
Under a general anaesthetic or occasionally a spinal anaesthetic, a cystoscope (bladder telescope) is passed up the urethra into the bladder and a very fine slippery flexible wire is passed under x-ray control up the ureter. The cystoscope is removed and the ureteroscope is then passed up the urethra through the bladder and up the ureter next to the guide wire under direct vision as well as x-ray control to the stone. If the ureter is very tight sometimes this may require dilatation to enable introduction of the ureteroscope. Small stones can be extracted in a fine wire basket and larger stones require vaporization/fragmentation using the holmium laser. A ureteric stent is then usually inserted under x-ray control. This is a fine hollow flexible polyurethane tube about 3mm in diameter which enables urine to drain freely from the kidney down into the bladder past any swelling or inflammation in the ureter resulting from stone impaction and instrumentation.
Again, under a general anaesthetic, a cystoscope is passed up the urethra into the bladder and a two fine slippery flexible wires are passed under x-ray control up the ureter. An access sheath, a long thin hollow tube is passed over one of the wires to act as a tunnel through which the flexible ureteroscope is passed to the upper ureter or kidney (pyeloscopy). Stones are vaporised/fragmented using the holmium laser, a delicate, demanding and time-consuming procedure. Again, a ureteric stent is then usually inserted under x-ray control.
There are no cuts or wounds following this surgery but it is normal to experience some discomfort and irritation on voiding for a short time post operatively relating to the urethral instrumentation. The presence of the ureteric stent typically also causes a degree of irritation. There is usually some blood in the urine and urinary frequency due to the soft coil of the stent in the bladder. Because there are no valves in this stent during voiding some urine refluxes up the stent and it is not uncommon to feel some transient discomfort in the loin after voiding. These symptoms are usually minor, settle with time and disappear completely when the stent is removed. The stent is usually left in place for about a week but may need to be longer if the ureter was more traumatised. Discharge from hospital is usually either the same day as surgery or the following morning.
Ureteric stents can be left with a fine nylon string attached that protrudes from the urethra. In this case, stent extraction is performed by patients at home by simply pulling the string. If no string is attached, a flexible cystoscopy is required to grasp the end of the stent and pull it out. This is a very brief day surgical procedure taking only a couple of minutes, requiring no anaesthetic and involving minimal discomfort. Very rarely there can be some loin pain after stent removal if the ureter has not healed enough or some stone fragments are caught up and if simple analgesia is insufficient hospitalisation could be briefly required.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}